- About Us
-
Academics
Schools
Programs
General Information
-
Faculty
The faculty members and researchers working at IIHMR University come from varied backgrounds including, but not limited to medicine, public health, management, economics, statistics, demography, human geography, social and behavioral sciences, rural development and pharmaceuticals.
-
Admissions
- Research
Publications & Journal
- Executive Education
- Training
- Placements
- Contact
- Blog
- Fee Payment
- NAAC
- IQAC
- NIRF
-
About Us
- About IIHMR University
- Board of Management
- Academic Council
- Board of Studies
- Research Board
- Institutional Review Board
- Finance & Audit Committee
- Departmental Research Committee
- Chairperson's Message
- President's Message
- IIHMR University Act
- Infrastructure
- Collaboration
- Ranking
- Board of Studies (School of Digital Health)
- Awards & Accolades
-
Academics
- Institute of Health Management Research
- School of Pharmaceutical Management
- ML Mehta School of Development Studies
- School of Digital Health
- SD Gupta School of Public Health
- MBA (Hospital and Health Management)
- MBA (Pharmaceutical Management)
- MBA (Healthcare Analytics)
- Master of Public Health
- Student Manual – Cohort 9 (2021-2023)
- Master of Public Health (Offered by Johns Hopkins Bloomberg School of Public Health, USA in cooperation with IIHMR University, Jaipur, India)
- PhD Programme
- MBA CSR & ESG Management (Executive)
- MBA Sustainable Business Management (Executive)
- Common Information for all the Programs
- Academic Calendar
- Student Handbook 2020-21
- Committees
- Policies
- Annual Exam Calendar
- Library
- Faculty
- Officers of University
- Dean of Institute of Health Management Research
- Dean of School of Pharmaceutical Management
- Dean of School of Development Studies
- Dean of SD Gupta School of Public Health
- Dean of School of Digital Health
- School of Digital Health
- Faculty List A to Z
- Faculty List Designation Wise
- Faculty List School Wise
- Admissions
- Research
- Executive Education
- Training
- Placements
- Alumni
- Events
- Job Openings
- Contact
- Research


Ebola Virus Outbreak
Ebola Virus Disease Outbreak
Update #9 Date- 24/07/2026
Occurrence Update
Democratic Republic of the Congo (DRC)
The Democratic Republic of the Congo remains the epicentre of the outbreak. As of 15 July 2026, a total of 2,124 confirmed cases and 828 deaths have been reported, resulting in a case fatality ratio (CFR) of 39%. A total of 390 patients has recovered. Since 3 July 2026, an additional 664 confirmed cases and 376 deaths have been recorded.
Uganda
As of 14 July 2026, Uganda has reported 20 confirmed cases, including two confirmed deaths among imported cases and one probable fatal case. Of the confirmed cases, 15 were imported from the Democratic Republic of the Congo, while five were secondary infections among healthcare workers and close contacts. Eighteen patients have recovered, and 821 of the 831 identified contacts have completed the required 21-day follow-up period. No community transmission has been detected, and Uganda has entered the 42-day enhanced surveillance period following the discharge of its last patient on 16 July 2026.
France
France has reported one imported case of Ebola disease caused by the Bundibugyo virus. The patient recovered completely and was discharged on 4 July 2026 after testing negative twice by polymerase chain reaction (PCR). All five identified flight contacts completed quarantine without developing symptoms, and no secondary transmission has been reported.
Germany
Germany has managed two imported cases involving United States citizens evacuated from the Democratic Republic of the Congo. The first patient recovered and was discharged, while the second patient, admitted in July 2026, remains in stable condition. No secondary cases have been reported.
Summary of Cases by Country
| Country | Confirmed Cases | Deaths | Recoveries | Current Situation |
|---|---|---|---|---|
| Democratic Republic of the Congo | 2,124 | 828 | 390 | Active outbreak with ongoing transmission |
| Uganda | 20 | 2 confirmed deaths and 1 probable death | 18 | No community transmission; under enhanced surveillance |
| France | 1 (imported) | 0 | 1 | Recovered; no secondary transmission |
| Germany | 2 (imported) | 0 | 1 recovered; 1 stable | No secondary transmission |
Update #8 Date- 06/07/2026
Occurrence Update
The Ebola disease outbreak caused by the Bundibugyo virus continues to expand, particularly in the Democratic Republic of the Congo (DRC). Since the previous outbreak update on 19 June 2026, there has been a rapid increase in confirmed cases and deaths. As of 2 July 2026, a total of 1,481 confirmed cases has been reported globally, including 1,460 cases from the Democratic Republic of Congo, 20 cases from Uganda, and one imported case in France. A total of 454 deaths has been recorded, including 452 deaths in the DRC and two in Uganda. Encouragingly, 229 patients have recovered, with 213 recoveries reported in the DRC and 16 in Uganda.
Democratic Republic of the Congo
The Democratic Republic of the Congo remains the epicentre of the outbreak. Since 19 June, an additional 564 confirmed cases and 220 deaths have been reported, partly due to expanded surveillance, increased testing, and improved laboratory capacity.
As of 1 July 2026, the country has reported 1,460 confirmed cases and 452 deaths, resulting in a case fatality rate (CFR) of approximately 31%. The outbreak has affected 36 health zones across the provinces of Ituri, North Kivu, and South Kivu. Among these, 21 health zones continue to report active transmission, while no new cases have been reported from the remaining areas during the past 21 days.
Ituri Province remains the most affected, accounting for over 91% of all confirmed cases and 84% of all deaths. The highest numbers of cases have been reported from Bunia, Rwampara, Mongbwalu, Nyankunde, and Nizi health zones. The outbreak has recently spread to additional areas, including Wamba (Haut Uele Province) and Kisangani (Tshopo Province), following the identification of infected individuals who had travelled from Nia Health Zone.
Healthcare workers continue to be significantly affected, with 102 confirmed infections and 25 deaths reported among medical and healthcare personnel. More than 10,800 contacts have been identified and placed under follow-up in the affected provinces. Most contacts are being monitored successfully, with follow-up rates exceeding 80%. In addition, 107 contacts linked to the imported case in France are also being monitored in Kinshasa.
The response continues to face major challenges due to ongoing conflict, population displacement, insecurity, and limited access to healthcare services. Overcrowded displacement camps, poor sanitation, and restricted movement of response teams increase the risk of further disease transmission and complicate outbreak control efforts.
Uganda
Uganda has reported a total of 20 confirmed Ebola cases, including two deaths, along with one probable fatal case. Of the confirmed cases, 15 were imported from the Democratic Republic of Congo, while five were secondary infections among contacts and healthcare workers exposed to imported cases.
Cases have been reported in Kampala and Wakiso District, both within the Kampala Metropolitan Area. Importantly, no community transmission has been documented, and the outbreak remains limited to imported infections and their close contacts. The last confirmed case was identified on 21 June 2026, and 16 patients have recovered. Nearly all identified contacts have successfully completed the required 21-day monitoring period.
France
On 24 June 2026, France reported its first imported case of Ebola disease caused by the Bundibugyo virus. The patient was a medical doctor who had recently returned after working for five weeks in Ituri Province, Democratic Republic of Congo, caring for Ebola patients.
Upon arrival at Charles de Gaulle Airport on 23 June, the doctor reported symptoms to airport health authorities and was immediately isolated and admitted to a specialized treatment facility. Laboratory testing confirmed Bundibugyo virus infection. The patient remained clinically stable without severe symptoms such as bleeding, vomiting, or diarrhoea during travel.
Contact tracing activities were immediately initiated in both France and the Democratic Republic of the Congo to identify and monitor individuals who may have been exposed.
References
Ebola Virus Disease Outbreak
Update #7 Date- 19/06/2026
Occurrence Update
Democratic Republic of the Congo & Uganda
Since the previous update issued on 13 June 2026, an additional 220 confirmed Ebola cases, including 96 deaths, have been reported in the Democratic Republic of the Congo (DRC). As of 17 June 2026, a cumulative total of 896 confirmed cases, including 232 deaths (CFR: 26%), have been reported across 33 health zones in three provinces: Ituri (21 of 36 health zones), North Kivu (11 of 35 health zones), and South Kivu (1 of 34 health zones). To date, 78 patients have recovered from the disease. Ongoing epidemiological investigations and expanded laboratory testing continue to identify previously undetected cases and reclassify earlier suspected infections and deaths.
The outbreak remains predominantly concentrated in Ituri Province, accounting for 91.1% (817/896) of all confirmed cases nationwide, with a CFR of 22.7% (186/817). Within Ituri, the highest numbers of confirmed cases have been recorded in Bunia (247 cases), Rwampara (195 cases), Mongbwalu (189 cases), and Nyankunde (68 cases) health zones. New cases have also been reported from four additional health zones, although investigations indicate that transmission had likely been occurring in some of these areas for several weeks before confirmation.
As of 17 June 2026, a total of 6,367 contacts have been identified and placed under active follow-up across Ituri (4,659 contacts), North Kivu (1,628 contacts), and South Kivu (80 contacts). Overall contact follow-up rates have reached approximately 71% in Ituri and North Kivu and 100% in South Kivu.
Response operations continue to face considerable challenges due to the complex humanitarian and security situation in the affected provinces. High population mobility, internal displacement, limited access to essential services, and increasing security incidents affecting health facilities have disrupted surveillance and response activities and increased the risk of undetected transmission.
Uganda
As of 18 June 2026, Uganda has reported a cumulative total of 19 confirmed Ebola cases, including two deaths, and one probable case who also died. No new cases have been reported since 5 June 2026. To date, 10 patients have recovered from the disease.
Cases remain epidemiologically linked to transmission originating in the Democratic Republic of the Congo, with evidence of both imported infections and secondary transmission among contacts and healthcare workers. Reported cases have included cross-border travellers, healthcare workers, and individuals with epidemiological links to previously confirmed cases.
National authorities, in collaboration with WHO and partners, continue to implement surveillance, contact tracing, infection prevention and control (IPC) measures, and cross-border coordination activities. Although no new cases have been reported in recent weeks, the continued risk of cross-border transmission necessitates sustained vigilance and preparedness efforts.
Ebola Virus Disease Outbreak
Update #6 Date- 15/06/2026
Occurrence Update
Democratic Republic of the Congo
Since 8 June 2026, an additional 161 confirmed cases, including 45 deaths, have been reported in the Democratic Republic of the Congo (DRC). This increase is partly attributable to the expansion of laboratory testing and diagnostic capacity, which has facilitated the analysis of previously collected samples that were awaiting confirmation. As of 10 June 2026, the DRC has reported a cumulative total of 676 confirmed cases and 136 deaths, resulting in a case fatality rate (CFR) of 20.1%. However, the actual CFR may be higher, as several deaths that occurred prior to the official outbreak declaration remain under investigation. To date, 32 patients have recovered.
Confirmed cases have been reported across 29 health zones (HZs), including 19 of 36 HZs in Ituri Province, 9 of 35 HZs in North Kivu Province, and 1 of 34 HZs in South Kivu Province. Sixteen confirmed infections have occurred among health and care workers.
The outbreak continues to be concentrated in Ituri Province, which accounts for 93% (629/676) of all confirmed cases. The province has reported a CFR of 17.3% (109 deaths among 629 confirmed cases). The highest numbers of confirmed cases have been recorded in the health zones of Bunia (185 cases), Rwampara (137 cases), Mongbwalu (132 cases), and Nyankunde (33 cases). Although Ituri remains the outbreak epicentre, there has been notable geographic expansion since 8 June, with four additional health zones reporting confirmed cases by 10 June. Furthermore, 94 confirmed cases are still awaiting allocation to specific health zones.
As of 10 June, a total of 5,768 contacts had been identified and placed under active follow-up across the affected provinces, including 4,703 in Ituri, 841 in North Kivu, and 224 in South Kivu. Among these, 4,141 contacts were successfully followed up, corresponding to follow-up rates of 71.4% in Ituri, 71.0% in North Kivu, and 83.5% in South Kivu.
The outbreak is occurring in a complex humanitarian setting marked by ongoing conflict, population displacement, and high levels of population mobility. These factors, coupled with increasing security-related incidents affecting health facilities, continue to create substantial operational challenges for outbreak response efforts. Restricted access to affected areas, disruptions to surveillance and response activities, and an increased risk of undetected transmission remain major concerns. These circumstances highlight the critical importance of community-centred interventions and strong engagement with local leaders to ensure an effective and sustainable response.
Ebola Virus Disease Outbreak
Update #5 Date- 10/06/2026
Occurrence Update
Democratic Republic of the Congo
Since 29 May 2026, an additional 390 confirmed cases, including 74 deaths, have been reported in the Democratic Republic of the Congo (DRC). This increase is partly attributable to the expansion of testing and diagnostic capacities, which enabled the processing of previously collected samples awaiting analysis. As of 6 June 2026, a cumulative total of 515 confirmed cases and 91 deaths have been reported, resulting in a case fatality rate (CFR) of 17.7%. However, the CFR may be underestimated, as several deaths that occurred prior to the official outbreak declaration are still under investigation. To date, 12 patients have recovered from the disease.
Cases have been identified across 25 health zones (HZs), including 17 of 36 HZs in Ituri Province, 7 of 35 HZs in North Kivu Province, and 1 of 34 HZs in South Kivu Province. Sixteen confirmed cases have occurred among health and care workers.
The outbreak remains predominantly concentrated in Ituri Province, which accounts for 94% (487/515) of all confirmed cases. The CFR in Ituri stands at 15% (74/487), considerably lower than the 64% (16/25) CFR reported in North Kivu. Within Ituri, the highest numbers of confirmed cases have been reported from Bunia (142 cases), Rwampara (98 cases), Mongbwalu (92 cases), and Nyankunde (24 cases) health zones.
As of 6 June, a total of 5,040 contacts had been identified and placed under monitoring across the affected provinces, including 4,118 in Ituri, 699 in North Kivu, and 223 in South Kivu. During the preceding 24 hours, 2,535 contacts were successfully followed up, corresponding to follow-up rates of 43.2% in Ituri, 82.5% in North Kivu, and 80.3% in South Kivu.
The response continues to face significant operational challenges due to increasing security-related incidents affecting health facilities in the affected areas. These disruptions limit access for response teams, hinder surveillance and case management activities, and heighten the risk of undetected disease transmission. The situation underscores the importance of sustained engagement with local leaders and communities to support outbreak control efforts and maintain essential public health operations.
Uganda
Since the previous update on 29 May 2026, Uganda has reported an additional 10 confirmed cases and one death. As of 6 June 2026, the country has recorded a total of 19 confirmed cases, including two deaths among imported cases, as well as one probable case who died. Five patients have recovered to date.
Of the 19 confirmed cases, 14 are imported cases and five are Ugandan nationals. Cases have been identified in two districts, Kampala and Wakiso. All reported cases have been epidemiologically linked either to travellers arriving from the Democratic Republic of the Congo (DRC) or to secondary transmission associated with these imported cases. No evidence of community transmission has been documented in Uganda. Current exposure risks are primarily linked to healthcare settings and cross-border population movement.
Approximately 70% of the confirmed cases are Congolese nationals who entered Uganda seeking medical treatment. Among these was a Congolese national who travelled from the DRC through Uganda to the United Arab Emirates (UAE) and subsequently returned to Uganda. The World Health Organization (WHO), in collaboration with public health authorities in Uganda and the UAE, is gathering additional information to assess potential exposure risks and support contact-tracing efforts through the National International Health Regulations (IHR) Focal Point mechanism.
Based on available information, there is no indication that the individual exhibited symptoms clearly consistent with Bundibugyo Virus Disease (BVD) during travel to or from the UAE. Following notification of the case, UAE authorities promptly initiated risk assessments, contact tracing, monitoring of identified contacts, public health investigations, enhanced preparedness measures at points of entry, and coordination with national and international partners.
Epidemiological investigations conducted thus far have not detected any secondary cases, local transmission, or evidence of onward spread within the UAE. These findings indicate that the risk of transmission associated with this event in the UAE remains low.
As of 2 June 2026, a total of 668 contacts linked to confirmed cases had been identified and placed under active follow-up. These contacts include household members, close residential contacts, and healthcare-associated contacts from facilities where cases received treatment.
Ebola Outbreak
Update #4 Date- 30/05/2026
Occurrence update
Democratic Republic of the Congo
Since the previous update issued on 21 May 2026, an additional 42 confirmed Ebola cases, including eight deaths, and 160 suspected cases, including 47 deaths, have been reported in the Democratic Republic of the Congo (DRC). As of 27 May 2026, a cumulative total of 125 confirmed cases, including 17 deaths and 906 suspected cases, including 223 deaths, have been reported across 13 health zones in three provinces: Ituri (7 of 36 health zones), North Kivu (5 of 35 health zones), and South Kivu (1 of 34 health zones). To date, 16 confirmed infections have been identified among health and care workers. Ongoing epidemiological investigations and laboratory testing are being conducted to verify and reclassify suspected cases and deaths.
The outbreak continues to be predominantly concentrated in Ituri Province, which accounts for 88% (110/125) of all confirmed cases reported nationwide. Within Ituri, the highest numbers of confirmed cases have been recorded in Bunia (37 cases), Rwampara (33 cases), Mongbwalu (20 cases), and Nyankunde (10 cases) health zones. Among the 17 confirmed deaths, 10 occurred in males (nine aged over 15 years and one under 15 years), while seven occurred in females (five aged over 15 years and two under 15 years).
Contact tracing efforts have identified 2,635 contacts across Ituri and North Kivu provinces as of 27 May 2026. Response operations continue to face significant challenges, particularly in Ituri Province, where recent security incidents targeting health facilities and increasing community resistance have been reported in Mongbwalu and Rwampara health zones.
Uganda
Since the previous update issued on 21 May 2026, seven additional confirmed Ebola cases have been reported in Uganda. As of 29 May 2026, the country has recorded a cumulative total of nine confirmed cases, including one death. Cases have been reported from Kampala District (n=8) and Wakiso District (n=1).
Recent confirmed cases include a Ugandan truck driver who had transported the index case, a Congolese healthcare worker epidemiologically linked to the initial case, a Congolese woman who travelled to Uganda seeking medical treatment, and two Ugandan healthcare workers associated with previously confirmed cases. These findings indicate ongoing transmission linked to both healthcare settings and cross-border population movement.
As of 26 May 2026, a total of 436 contacts had been identified and placed under active follow-up. These contacts include household members, healthcare workers, and individuals exposed within healthcare facilities where confirmed cases received treatment.
The current outbreak highlights the continued risk of transmission through healthcare-associated exposure and cross-border travel. Strengthened surveillance, rigorous contact tracing, infection prevention and control (IPC) measures in healthcare facilities, and enhanced cross-border coordination remain critical to limiting further spread.
Ebola Outbreak
Update #3 25/05/2026
Occurrence update
Since the previous Outbreak News published on 16 May 2026, the number of suspected and confirmed cases in the Democratic Republic of the Congo (DRC) has risen rapidly, with the outbreak spreading geographically into North Kivu and South Kivu provinces. As of 21 May 2026, the DRC had reported a total of 746 suspected cases, including 176 deaths among suspected cases. Across both the DRC and Uganda, 85 confirmed cases, including two cases in Uganda, and ten confirmed deaths, including one in Uganda, have been reported.
Democratic Republic of the Congo
As of 21 May 2026, the Democratic Republic of the Congo (DRC) had reported a total of 83 confirmed Ebola cases, including nine deaths. In addition, 746 suspected cases, including 176 deaths, have been reported across 15 health zones in Ituri, North Kivu, and South Kivu provinces. To date, four deaths have been reported among healthcare workers. Ongoing epidemiological and laboratory investigations are being conducted to verify and reclassify suspected cases and deaths reported in the country.
The most affected health zones are Mongbwalu, Rwampara, and Bunia, which together account for 96% of suspected cases and 79% of confirmed cases.
An American national working as a surgeon in the DRC has also been confirmed to have Ebola virus disease. The exposure is believed to have occurred during a medical procedure performed on 11 May 2026. Symptoms reportedly began on 16 May, and laboratory confirmation was obtained on 20 May. The patient is currently receiving treatment in a high-level isolation unit in Berlin, Germany.
Response efforts continue to face several significant challenges, including the lack of standardized isolation and treatment facilities, as well as weak screening and referral systems. Inconsistent implementation of safe and dignified burial practices continues to increase the risk of healthcare-associated transmission. Cross-border transmission also remains a major concern due to ongoing insecurity, humanitarian crises, high population mobility, urban and semi-urban transmission hotspots, and porous international borders, highlighting the need for strengthened surveillance and enhanced cross-border information sharing.
Affected communities are facing increasingly difficult conditions, with growing concerns regarding access to free and supportive healthcare services, the availability of respectful and dignified burial practices, and the spread of misinformation and rumours. In addition, ongoing conflict in Ituri Province continues to hinder outbreak response activities by restricting the movement of surveillance teams, delaying the deployment of Rapid Response Teams, and affecting the transportation of laboratory samples.
Uganda
As of 20 May 2026, Uganda had reported two confirmed Ebola cases, including one death, both linked to importation from the Democratic Republic of the Congo (DRC). The first confirmed case was admitted to a private hospital in Kampala on 11 May and subsequently died on 14 May. The body was repatriated to the DRC on the same day.
The second confirmed case was identified on 16 May in Kampala in an individual who had recently returned from the DRC and had no known epidemiological connection to the first case. The patient is currently receiving treatment at the Mulago Isolation Treatment Unit in Uganda. As of the reporting date, no evidence of local transmission has been detected in Uganda.
As of 18 May 2026, a total of 127 contacts linked to the two confirmed imported cases had been identified and were under active follow-up. These contacts include household members, close personal contacts, and healthcare workers or patients exposed in the healthcare facilities where the cases received treatment.
The risk of exposure remains associated with both healthcare settings and cross-border population movements. On 18 May, authorities reported and investigated 18 alerts related to suspected Ebola cases. Additionally, four active cross-border exposure clusters identified in Ntoroko District are currently under investigation to assess potential transmission risks and strengthen containment measures.
References
Ebola Outbreak
Update #2 21/05/2026
Occurrence update
On May 17, a United States national who had been exposed to Ebola Bundibugyo disease while providing patient care in the Democratic Republic of the Congo (DRC) tested positive for the infection. The individual was transferred to Germany for specialized treatment and clinical management, as Germany has prior experience in handling Ebola cases and offers a shorter transport time for medical evacuation.
Several high-risk contacts linked to this exposure have also been relocated to Germany and Czechia for monitoring and preventive management. At present, no additional Ebola cases have been identified among U.S. nationals.
According to updates released on May 19 by the Ministries of Health of the DRC and Uganda, the outbreak situation includes:
- 536 suspected cases
- 105 probable cases
- 34 confirmed cases
- 134 suspected deaths
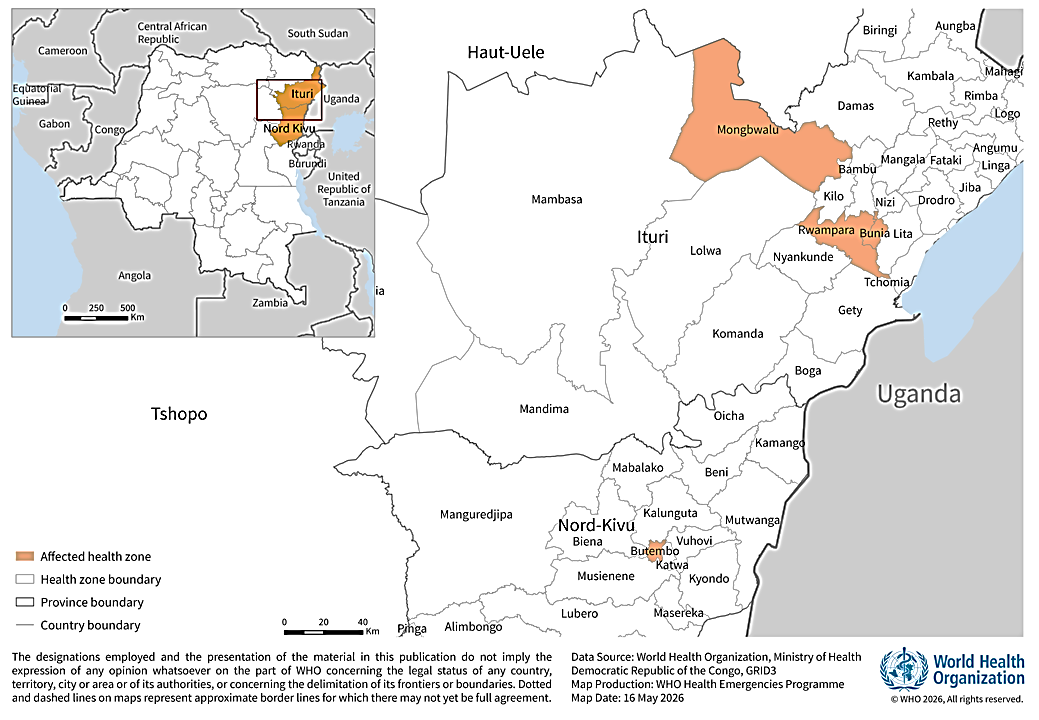
Source- WHO- Health Zones affected by Bundibugyo virus disease in Democratic Republic of Congo
Within the previous 24–48 hours, health authorities reported 26 newly confirmed cases and 143 additional suspected cases, indicating continued transmission and active surveillance efforts.
The reported figures also include two confirmed cases in Uganda, one of which resulted in death, involving individuals who had recently travelled from the DRC. No evidence of further transmission within Uganda has been documented so far.
The situation remains highly dynamic, and epidemiological data may continue to change as investigations and laboratory confirmations progress.
On May 18, the Centers for Disease Control and Prevention, in collaboration with the Department of Homeland Security and other federal agencies, implemented precautionary public health and travel-related measures aimed at reducing the risk of Ebola importation into the United States. Additional details regarding enhanced travel screening and security protocols are expected to be released.
Despite these developments, public health authorities continue to assess the overall risk of Ebola transmission to the United States as low.
India’s Current Actions on the Ebola Outbreak (May 2026)
India has strengthened its preparedness and response measures following the recent Ebola outbreak in affected African countries such as the Democratic Republic of the Congo (DRC) and Uganda. Enhanced airport screening has been initiated for passengers arriving from or transiting through affected regions, while travel advisories have been issued asking travellers to immediately report symptoms such as fever, vomiting, bleeding, or weakness and seek medical care if symptoms develop after travel. The Union Health Ministry has conducted high-level review meetings with all states and Union Territories to assess preparedness and response capacity. Surveillance systems have been strengthened through the Integrated Disease Surveillance Programme (IDSP), the National Centre for Disease Control (NCDC), and airport and port health authorities. Laboratory preparedness has also been enhanced, with the National Institute of Virology designated as a key Ebola testing center. Hospitals and isolation facilities across the country have been instructed to maintain adequate PPE supplies, infection prevention and control measures, and rapid response readiness. In addition, healthcare workers have been sensitized and trained regarding early symptom detection, infection prevention and control practices, safe sample handling, and contact tracing procedures.
Reference
- https://www.cdc.gov/ebola/situation-summary/index.html
- https://indianexpress.com/article/health-wellness/ebola-alert-health-ministry-airport-screening-surveillance-lab-preparedness-10696700/?utm
- https://indianexpress.com/article/health-wellness/ebola-alert-health-ministry-airport-screening-surveillance-lab-preparedness-10696700/lite/?utm
- https://timesofindia.indiatimes.com/india/india-tightens-ebola-surveillance-at-airports-issues-health-advisory-for-travellers-from-african-nations/articleshow/131240702.cms?utm
Ebola Virus Outbreak
Update #1 16/05/2026
Occurrence update
On 5 May 2026, health authorities received an alert regarding an unidentified illness with a high fatality rate in the Mongbwalu Health Zone of Ituri Province, Democratic Republic of Congo. The alert included reports of four health workers who died within a period of four days. Following field investigations conducted by rapid response teams in the Mongbwalu and Rwampara health zones on 13 May, laboratory findings later confirmed the outbreak as Bundibugyo Virus Disease (BVD) caused by the Bundibugyo virus species on 15 May 2026.
On the same day, the Ministry of Public Health, Hygiene and Social Welfare officially declared the 17th Ebola disease outbreak in DRC, affecting the Rwampara, Mongbwalu, and Bunia health zones.
The earliest known suspected case was a health worker who developed symptoms including fever, bleeding, vomiting, and severe weakness on 24 April 2026. The patient later died at a medical facility in Bunia.
As of 15 May 2026, approximately 246 suspected cases and 80 deaths, including four among laboratory-confirmed cases, had been reported from the affected health zones. Twenty-four suspected cases were being managed in isolation facilities across the three health zones. In addition, investigations are ongoing into several clusters of unexplained community deaths with symptoms consistent with Bundibugyo Virus Disease in other areas of Ituri and North Kivu provinces.
Most suspected cases have been reported among individuals aged 20–39 years, with women accounting for more than 60% of cases, indicating a possible increased risk related to caregiving and household exposure.
Initial laboratory testing of 20 samples collected from Rwampara Health Zone at the Provincial Public Health Laboratory in Bunia returned negative results using standard Ebola Xpert testing. However, further testing at INRB confirmed eight samples positive for Ortho ebolavirus by polymerase chain reaction (PCR) on 15 May 2026. Genomic sequencing later identified the virus as Bundibugyo virus (BDBV). Bundibugyo Virus Disease is caused by the Bundibugyo virus (BDBV), a member of the Orthoebolavirus genus under the Filoviridae family. It is one of the three Ebola virus species known to cause severe disease and outbreaks in humans, along with Ebola virus (EBOV) and Sudan virus (SUDV). Currently, no licensed vaccine or specific treatment is available for Bundibugyo Virus Disease, although research and development of candidate vaccines and therapeutics are ongoing.
As of 15 May, a total of 65 contacts had been identified, including 15 categorized as high-risk contacts. Contact follow-up activities remain challenging due to insecurity and movement restrictions in the affected areas. Several listed contacts reportedly developed symptoms and died before they could be isolated.
On 15 May 2026, the Uganda Ministry of Health confirmed an outbreak of Bundibugyo Virus Disease after detecting an imported case from DRC. The case involved an elderly man who was admitted to a private hospital on 11 May with severe symptoms and died on 14 May. His body was later transferred back to DRC on the same day. Laboratory testing of samples collected during admission confirmed Bundibugyo virus infection on 15 May. A second imported case was confirmed in Kampala on 16 May in an individual returning from DRC who had no known epidemiological link to the first case. At the time of reporting, no local transmission had been identified in Uganda.
Current investigations suggest that the outbreak may have originated in the Mongbwalu Health Zone, a densely populated mining area with high levels of population movement. Cases are believed to have subsequently spread to Rwampara and Bunia as affected individuals travelled to seek medical care. Ituri Province shares borders with Uganda and South Sudan, while Bunia is located less than 500 kilometres from Uganda. Epidemiological investigations and trace-back activities remain ongoing.
The role of Ituri as a major commercial and migration hub, along with its proximity to Uganda and South Sudan, continues to increase the risk of regional spread and cross-border transmission.
What is Ebola Virus?
Ebola disease is a rare but serious viral illness that affects humans and is associated with high mortality rates if not detected and managed early. The disease is caused by viruses belonging to the Orthoebolavirus genus under the Filoviridae family.
There are 3 types of orthoebolaviruses that cause illness in people:
- Ebola virus (species Orthoebolavirus zairense) causes Ebola virus disease.
- Sudan virus (species Orthoebolavirus sudanense) causes Sudan virus disease.
- Bundibugyo virus (species Orthoebolavirus bundibugyoense) causes Bundibugyo virus disease.
Three other types of orthoebolaviruses have not affected people to date:
- Reston virus (species Orthoebolavirus restonense) has caused disease in non-human primates like macaques.
- Taï Forest virus (species Orthoebolavirus taiense) causes Taï Forest virus disease
- Bombali virus (species Orthoebolavirus bombaliense) was more recently identified in bats.
The first recorded outbreaks of Ebola disease occurred in 1976 through two simultaneous events in Africa. One outbreak, caused by Sudan virus, occurred in Nzara in present-day South Sudan, while the second outbreak, caused by Ebola virus, occurred in Yambuku in what is now the Democratic Republic of Congo. The disease was later named after the nearby Ebola River.
At present, licensed vaccines and specific therapeutics are available for Ebola Virus Disease caused by EBOV. However, no approved vaccine or targeted treatment is currently available for other forms of Ebola disease such as Sudan Virus Disease or Bundibugyo Virus Disease, although several candidate vaccines and therapeutics are under development.
Early detection and timely supportive management, including rehydration, symptom management, and intensive clinical care, can significantly improve patient survival. Prompt medical attention remains critical for reducing complications and saving lives.
Transmission
Fruit bats are believed to be the natural hosts of the Ebola disease virus. Humans can become infected through contact with infected animals or their body fluids. The disease also spreads from person to person through direct contact with blood, body fluids, or contaminated objects. Infected individuals can transmit the virus only after symptoms appear. Healthcare workers and people involved in unsafe burial practices are at higher risk of infection.
Symptoms
Ebola disease usually starts suddenly with symptoms such as fever, weakness, fatigue, headache, muscle pain, and sore throat. As the disease progresses, patients may develop vomiting, diarrhoea, abdominal pain, and skin rash. In severe cases, bleeding from the nose, gums, or gastrointestinal tract may occur. The incubation period ranges from 2 to 21 days, with symptoms commonly appearing within 8–10 days after exposure. Some patients may also develop confusion, irritability, and other neurological symptoms.
Diagnosis
Diagnosing Ebola disease during the early stages can be challenging because its initial symptoms are similar to several other infectious diseases such as malaria, typhoid fever, shigellosis, meningitis, and other viral haemorrhagic fevers. Symptoms like fever, weakness, headache, and vomiting often overlap with these illnesses, making clinical identification difficult without laboratory testing.
Confirmation of Orthoebolavirus infection requires specialized laboratory investigations. Common diagnostic methods include:
- Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) testing
- Antibody-capture Enzyme-Linked Immunosorbent Assay (ELISA)
- Antigen detection tests
- Virus isolation through cell culture techniques
Laboratory confirmation is essential for accurate diagnosis, timely case management, and implementation of infection prevention and outbreak control measures.
Treatment
Management of Ebola disease mainly depends on early supportive care to improve patient survival. Treatment includes rehydration, pain management, nutritional support, monitoring of vital signs, and treatment of co-infections such as malaria and bacterial infections. Early medical care can significantly improve recovery outcomes. For Ebola Virus Disease (EVD) caused by Ebola virus (EBOV), monoclonal antibody therapies such as Ansuvimab and Inmazeb are available and recommended. However, no approved specific treatment currently exists for Sudan Virus Disease (SVD) or Bundibugyo Virus Disease (BVD), although research on new therapies is ongoing.
Vaccines
Approved vaccines are available for Ebola Virus Disease caused by the Ebola virus (EBOV), including Ervebo and the Zabdeno–Mvabea vaccine regimen. These vaccines are mainly used during outbreak response and for protecting healthcare and frontline workers in high-risk areas. However, no licensed vaccines are currently available for Sudan Virus Disease (SVD) or Bundibugyo Virus Disease (BVD). Several candidate vaccines for these diseases are under development and undergoing clinical evaluation.
Prevention
Community participation is very important for controlling Ebola disease outbreaks. Effective response measures include early treatment, surveillance, contact tracing, laboratory testing, infection prevention, safe burials, and public awareness activities. People should avoid contact with infected animals such as bats and monkeys, as well as direct contact with infected persons and their body fluids. Suspected patients should be isolated and treated in designated healthcare facilities to prevent further spread. Clear communication and community involvement help improve awareness, trust, and cooperation during outbreaks. Monitoring contacts for 21 days, maintaining hygiene, and following infection control measures are essential to stop transmission.
References
x
x